In early 1940s, well before the infamous Pruitt-Igoe housing complex would be built and destroyed just a few blocks south-east, another North Central St. Louis neighborhood stood condemned. Carr Square was known by its nickname “the lung block” for its high rates of tuberculosis deaths, and had been designated a blighted neighborhood to be torn down in one of the first slum-clearing projects in St. Louis made possible by the federal New Deal.

Taylor Desloge, a PhD student in history at WashU, researches the DeSoto-Carr neighborhood and how it became known as the lung block. What he has uncovered reveals complex urban history not only about housing discrimination and redlining, but also about public health narratives that have presented African Americans as a diseased community in need of containment. He looks at how the New Public Health movement played a central role in creating the very concept of blight by presenting social ills as located within specific geographic boundaries. This paved the way for the kind of displacement and disinvestment that Desloge says is central to 20th-century urban policy.
Desloge’s project uses property records to trace the history of the Carr neighborhood to its rural roots in the 19th century. Tracking property records is a painstaking and time-consuming process, but it produces an interesting story about the urbanization of the area. Desloge explains how immigrants who came into the neighborhood in the late 19th century bought up properties from old estate families that would later become sources of income to them as the city became more industrialized. “They begin subdividing what were single-family homes into tenements, and they begin renting out those homes to newer immigrants who are arriving in St. Louis,” he notes, “and they make a lot of money.”

As living units became smaller and people lived closer together, however, diseases like tuberculosis were able to spread more easily. Often residents shared inadequate restrooms with several different families, creating a perfect environment for the spread of disease. Progressive reformers of the 19th century began to push for housing improvements, but this movement fell apart as wealthier residents began to move to areas like the Central West End and University City. Desloge’s project tracks how early attempts at reform, which understood tuberculosis to be a problem of urbanization, fell apart, and how both property decline and tuberculosis slowly came to be closely associated with race.

In the 1910s, African Americans began entering St. Louis in large numbers as part of the Great Migration and provided an easy scapegoat for the decline of property values. Desloge explains that “just at the moment when tenement reform is failing, you get this influx of African American migrants, …and they sort of become the face of this decline of the property market in North St. Louis… a problem that was preexisting.” He notes that the entry of African American migrants took place in the context of two important events: the 1916 racial zoning referendum that sought to legally restrict housing in certain areas to specific races but was quickly deemed illegal, and the East St. Louis massacres of 1917 in which white industrial workers rioted and murdered many African Americans who they felt were taking their jobs. Both of these events contributed to the St. Louis Real Estate Exchange, a group of professional realtors, deciding in the early 1920s not to sell or rent real estate to African Americans outside of a small area in North St. Louis that included Carr Square.
Tuberculosis was already a problem in tenement buildings, but as the Real Estate Exchange’s decision to only sell property to African Americans in North St. Louis shifted the demographics of Carr Square from a mixed immigrant community to one that was predominantly African American, the disease became more closely associated with African Americans than with the area they lived in. As Desloge writes in his article on DeSoto-Carr, “From the perspective of the New Public Health as well as in the eyes of the public at large, DeSoto-Carr’s racial transition was the key factor of its emergence as a lung block.”

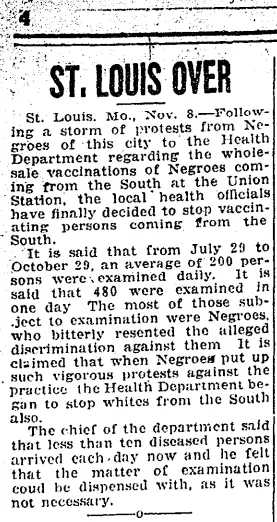
from which Desloge learned that African Americans were
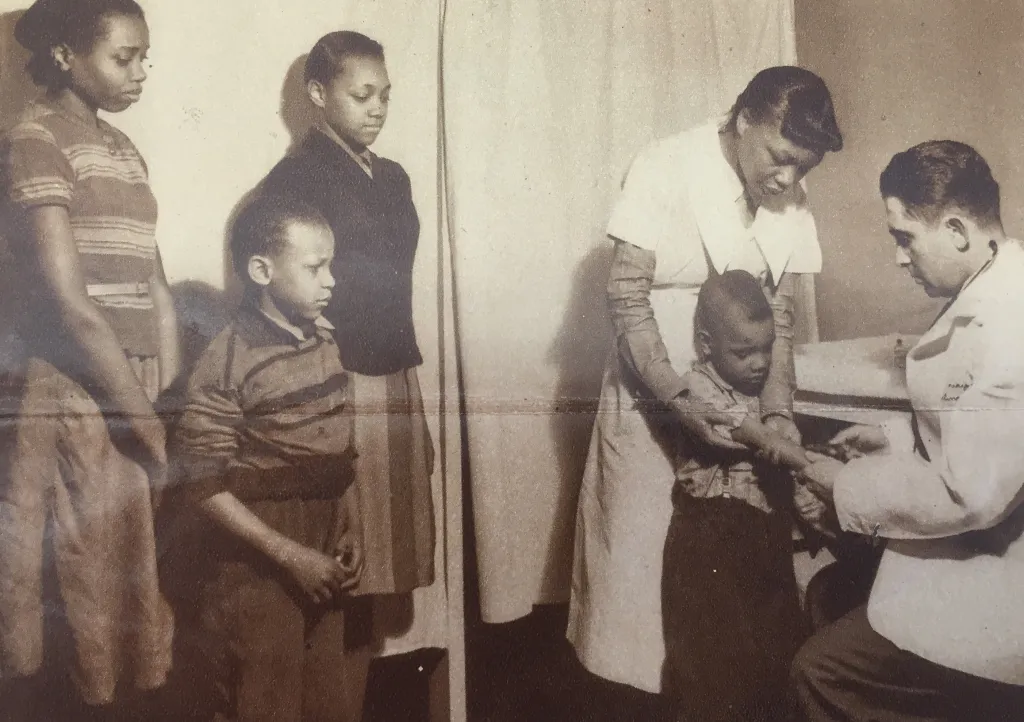
being forcibly vaccinated
St. Louis officials were so convinced of the link between African Americans and tuberculosis that they actually initiated a sort of quarantine for all black migrants who were coming into the city. In the course of his research, Desloge found a short article from the Baltimore Afro-American that reported that the St. Louis Health Department was forcing African Americans traveling from the South to undergo medical examinations and vaccinations when they arrived at Union station. “I discovered this… and I thought, that’s interesting. You normally associate quarantines and kinds of measures like that with national boarders,” he explains, “but I had never heard of that happening in a city before, of that happening with interstate migration rather than national migration.”
His curiosity sparked, Desloge dug further in the archives to find out why African Americans were being targeted by health officials more than their white peers. He found the shaping, in the 1920s and 1930s, of a complex narrative that associated African Americans with diseases like tuberculosis. This discovery has formed the basis of his recent article on the Lung Block that illuminates how fears of diseased black bodies contributed to the present-day racial segregation of St. Louis.
According to Desloge, there are many factors that contributed to a shift in the public perception of tuberculosis from a “disease of civilization” to one located specifically in black bodies, but one factor was a changing perception of public health. The New Public Health movement that took off in St. Louis in the 1910s and 1920s reoriented the field of public health, which had previously been focused on improving health environmental reform, toward a more strictly biological model of disease that targeted specific pathogens and their carriers.
The shift toward a biological model of disease allowed health officials to focus on the higher prevalence of tuberculosis among African Americans divorced from its environmental and social context. Property owners in tenement areas that the Real Estate Exchange had opened to black occupancy were so convinced of the link between African Americans and depreciating property values that they stopped investing in these tenements when demographics began to shift and neglected to make repairs or install amenities like plumbing. These depreciating living conditions of course led to higher incidents of tuberculosis, but because the New Public Health was less reform-oriented in its biological approach to illness, it failed to see the impact that environmental conditions were having on the spread of disease. “By shifting the focus to managing disease through control of microbes,” Desloge writes, “scientific public health began to shift the burden for disease onto patients themselves.”
The New Public Health movement is often framed as a positive example of medical progress toward a more objective, scientific perspective on disease, but Desloge argues that we need to examine this shift within the context of the time period in which it takes place, during which there were intense racial tensions between black migrants and white industrial workers that included the deadly 1917 East St. Louis riots. These racial biases tainted the medical narratives being spread by the New Public Health. Desloge writes that it should not be surprising that “as the New Public Health increasingly drew on social science during the 1920s and 1930s, discourses about health and neighborhood racial and economic transition started to sound remarkably similar.”
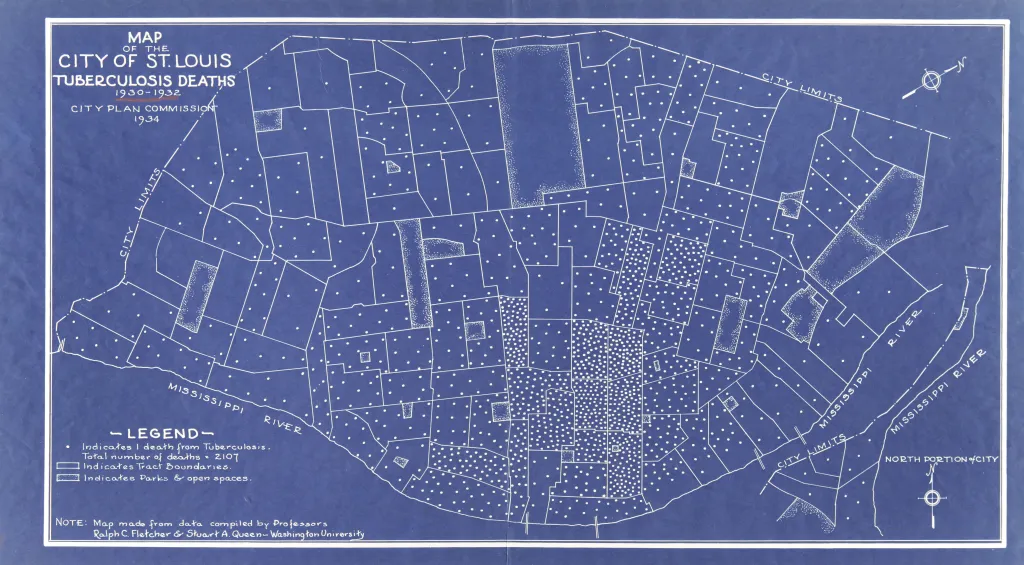
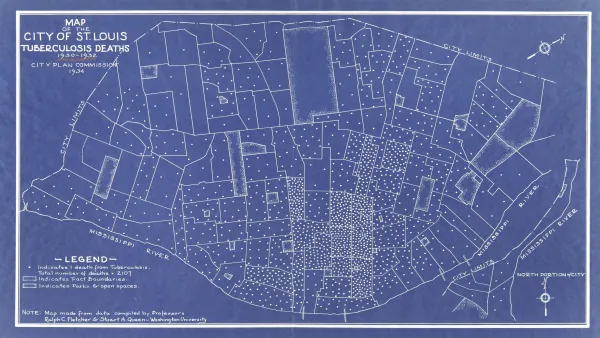
In the 1920s, the health department created pin maps to visually represent tuberculosis deaths in certain geographic areas. A large concentration of pins in the area of Carr Square led to this region being nicknamed “The Lung Block,” and cemented the idea that tuberculosis could be contained to certain “blighted” areas of the city occupied by African Americans.
The fear that this so-called blight would spread to infect white neighborhoods contributed to further racial segregation, and even provided a foundation for federal redlining by the Home Owner’s Loan Corporation (HOLC), a New Deal federal agency designed to insure mortgages. The HOLC used both tuberculosis and “negro encroachment” as signs of neighborhood instability, and denied certain financial and neighborhood services to residents of this area. DeSoto-Carr was eventually torn down during the New Deal as part of a slum clearance project.
Although Desloge’s current project ends with the 1940 slum clearance and the Carr Square Village project that was built on top of it, he sees connections between his work and later failed urban developments based in narratives of containment and segregation, such as Pruitt- Igoe. He writes, “I consider Pruitt Igoe to be part of the extended story of my research in a way, as my work is about the road to the kind of thinking that spatialized social ills and made the displacement and urban renewal projects of the postwar era seem like logical solutions.”
A project of this nature requires immense archival work, none of which he claims would have been possible without the guidance of his late mentor and main advisor, Maggie Garb, who passed away in December. Desloge repeatedly noted Garb’s influence on his work, stating, “Maggie taught me everything I know and I am really just incredibly grateful to her. She was a brilliant historian.”

One of the most important things Maggie taught him, however, has not been the technical skills he has used to do archival work, but the necessity of examining the past in order to change the future. “One of the things that Maggie really taught me was that there is nothing natural and nothing inevitable about racial segregation,” he says. “I always think about that, and I think that is what is at stake in my dissertation too. When you can see how something happened, how this happened, then you can see that it is not natural and inevitable and that it can be changed.”
Read more about the lung block in Desloge’s article, “Creating the Lung Block: Racial Transition and the Making of the ‘New Public Health’ in a St. Louis Neighborhood, 1907-1940” in the Missouri Historical Review. You can also read about his work on St. Louis’ Homer G. Phillips Hospital in his article, “The Separation Should Be Complete’: The Fight for Homer G. Phillips Hospital and the Making of a New Healthcare Politics in Interwar St. Louis,” in St. Louis Currents: Facing Regional Issues at 250.



